Pasteur Brewing Louis Pasteur – Science, Health, and Brewing
Pasteur Brewing Louis Pasteur – Science, Health, and Brewing Originally published online by with Richar G Fiddian-Green on CMAJ: Canadian Medical Association Journal, September 3, 2004
The Germ Theory was formulated by Louis Pasteur along with Robert Koch. The Germ Theory of disease states that “a specific disease is caused by a specific type of microorganism.” The theory gained strong support from the Viennese obstetrician, Dr. Ignac Semmelweis, who famously deduced that by not washing their hands between patients, or not washing them enough, doctors were actually to blame for puerperal fever, the leading cause of maternal death in hospitals. It gained further support from the formulation of Koch’s postulates, criteria for judging whether a given bacteria is the cause of a given disease. These postulates are:
- The specific organism should be shown to be present in all cases of animals suffering from a specific disease but shold not be found in healthy animals.
- The specific microorganism should be isolated from the diseased animal and grown in pure culture on artificial laboratory media.
- This freshly isolated microorganism, when inoculated into a healthy laboratory animal, should cause the same disease seen in the original animal.
- The microorganism should be reisolated in pure culture from the experimental infection.
Properly designed trials on hand disinfection have never demonstrated a reduction in either pneumonia and septicaemia, or mortality (1). “On the other hand, two meta-analyses have shown that selective decontamintion of the gut “reduces the odds ratio for lower airway infections to 0.35 (0.29- 0.41) and mortality to 0.80 (0.69-0.93), with a 6% overall mortality reduction from 30% to 24%. No increase in the rate of super infections due to resistant bacteria could be demonstrated over a period of 20 years of clinical research”.
It would appear, therefore, that nosocomial infections have an endogenous rather than an exogenous origin. The possibility remains, however, that endogenous organisms resistant to antibiotics might have been acquired in hospital. That does not, however, establish that that colonisation with these organisms [e.g. MSRA] is responsible for nosocominal infections in which they have been isolated.
It was the Canadian surgeons Meakins and Marshall who first drew attention to the possibility of the gut being the “motor of multiple organ failure”, the principle cause of late death in ICUs today(2). But nosocomial infections from gut organisms and indeed multiple organ dysfunction appears to be confined to patients whose gut mucosa has been compromised (3). In those who developed nosocomial pneumonias all appeared to have had an antecedent causal episode of gut mucosal compromise(4). Support for this finding was provided by a study in rabbits in which ischaemia/reperfusion injury of gastrointestinal mucosa was established to be the antecedent event (5). In patients having cardiovascular operations the ischaemia/reperfusion injury putative responsible for the nosocomial infections was the consequence of antecedent systemic disturbances, such as hypovolaemia, during the perioperative period rather than regional ones (6,7).
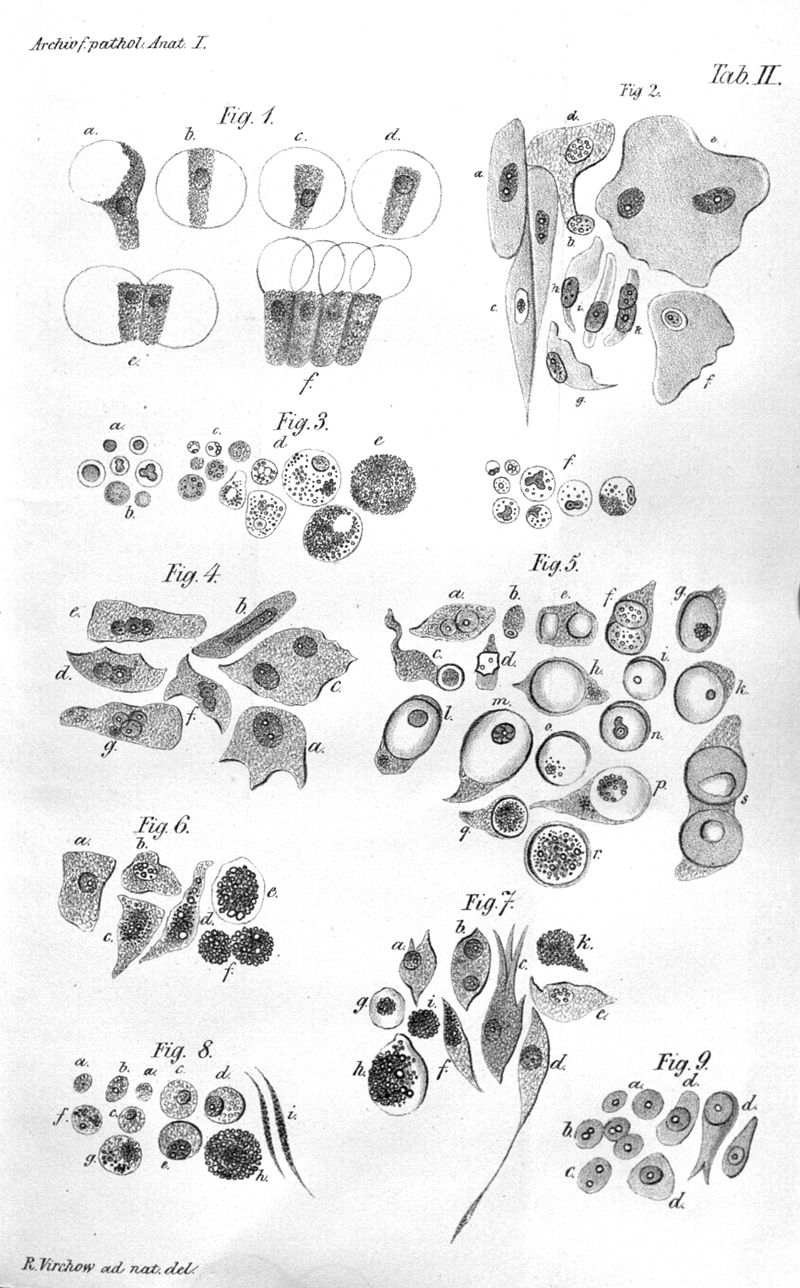
The Cell Theory was formulated by Matthias Schleiden, Theodor Schwann, and Rudolph Virchow. It stated:
- All living things are composed of one or more cells.
- Cells are organisms’ basic units of structure and function.
- Cells come only from existing cells.
Virchow, who never accepted the Germ Theory, was amongst the first to oppose the Greecian idea that disease was an affliction of the body at large or one of its Hippocratic humors wanting to find an antatomial origin. It was he who, according to Drotman at the Centers for Disease Control and Prevention in Atlanta, first established the principle that disease results from disturbed cellular function (8).
The energy charge hypothesis was first proposed by Daniel Atkinson in the 1960s (9). The system is activated in an ultrasensitive manner by cellular stresses that deplete ATP either by inhibiting ATP production (e.g. dehydration), or by accelerating ATP consumption (e.g. fever). The net effect is that cellular function is sacrificed to preserve cellular ATP and hence viability. It is in these circumstances that normal cellular function capable of resisting bacterial invasion, and its accompanying immunological defences, can be expected to be compromised by systemic disturbances in tissue energetics setting the stage for the Germ Theory to prevail.
The question arises, therefore, can Koch’s postulates ever be fulfilled in the absence of antecedent cellular dysfunction even in, for example, the case of diarrhoea caused by Shigella, Campylobacter and Entamoeba histolytica infections acquired in the tropics (10). Virchow’s Cell Theory would suggest not. What then of puerperal sepsis? Might it too be dependent upon antecedent cellular dyfunction caused by, for example, dehydration or hemorrhage? In other words might hand washing in obstetrics have no beneficial effect unless cellular function has been compromised by suboptimal attention to tissue energetics as must have been the norm in Semmelweis’s days?
I submit that Pasteur’s Germ Theory is subordinate to Virchow’s cell theory.
Footnotes
1. van Saene HK, Petros AJ, Ramsay G, Baxby D. All great truths are iconoclastic: selective decontamination of the digestive tract moves from heresy to level 1 truth. Intensive Care Med. 2003 May;29(5):677-90.
2. Meakins JL, Marshall JC: The gut as the motor of multiple system organ failure; in Marston A, Bulkley GB, Fiddian Green R.G (eds): Splanchnic Ischemia and Multiple Organ Failure. St Louis, CV Mosby, 1989, pp 339-348.
3. Fiddian-Green RG, Gantz NM Transient episodes of sigmoid ischemia and their relation to infection from intestinal organisms after abdominal aortic operations. Crit Care Med. 1987 Sep;15(9):835-9.
4. Fiddian-Green RG, Baker S Nosocomial pneumonia in the critically ill: product of aspiration or translocation? Crit Care Med. 1991 Jun;19(6):763-9.
5. Nielsen VG, Tan S, Baird MS, McCammon AT, Parks DA. Gastric intramucosal pH and multiple organ injury: impact of ischemia-reperfusion and xanthine oxidase. Crit Care Med. 1996 Aug;24(8):1339-44.
6. Fiddian-Green RG. Gut mucosal ischemia during cardiac surgery. Semin Thorac Cardiovasc Surg. 1990 Oct;2(4):389-99.
7. Bjorck M, Hedberg B Early detection of major complications after abdominal aortic surgery: predictive value of sigmoid colon and gastric intramucosal pH monitoring. Br J Surg. 1994 Jan;81(1):25-30.
8. D. Peter Drotman. Emerging Infectious Diseases: Special Issue. A Brief Biographical Heritage Emerging infectious diseases. Volume 4(3), July-Sepotmber 1998.
9. Hardie DG, Hawley SA. AMP-activated protein kinase: the energy charge hypothesis revisited. Bioessays. 2001 Dec;23(12):1112-9.
10. Butler T, Dahms B, Lindpaintner K, Islam M, Azad MA, Anton P Segmental necrotising enterocolitis: pathological and clinical features of 22 cases in Bangladesh. Gut. 1987 Nov;28(11):1433-8